
Why do hemiparesis patients need therapy when the damage is irreversible?
Hemiparesis is caused by a lesion in the central nervous system which means that the sensorimotor areas responsible for controlling movements are affected.
People with hemiparesis, just like people without a sensorimotor limitation, try to move both legs symmetrically for walking, relying on the information from their sensory system (like the proprioception). However, since this system is damaged, the patient receives incorrect and asymmetrical feedback about the current position of his or her joint position, muscle tension, weight distribution etc. Against this background, he
 or she cannot control and execute a symmetrical walking movement.
or she cannot control and execute a symmetrical walking movement.
Central nervous system lesions are irreversible, i.e. these structures cannot really be cured or restored.
Instead, specific therapeutic measures need be taken for the rehabilitation of patients with hemiparesis and similar diseases, which aim to transfer the tasks of the injured brain regions (here the movement control) to other systems. Even if the damage in the central nervous system cannot be cured, alternative control programs can be built up with a novel therapy which lead to significant improvements in the movement sequences. Without a therapy, a downward spiral often begins for patients, the negative consequences of which can go far beyond the original movement limitations caused by the disability.
The effect of such a spiral can be imagined as follows: Due to the disturbed control, non-symmetrical walking movements occur, which put too much strain on the joints and damage them on the long run, damages that cause severe pain. In addition, muscles are either overused, which leads to further tension and pain, or used too little, which in turn leads to the regression of muscles. This progression causes the asymmetry of the gait pattern and thus further limitations in movement, by which this cycle starts again. Ultimately, there are increasing spasticities, increasing immobility and, as a result, more sick leave, exclusion and, not infrequently, depression.
The rehabilitation approach by ReMoD
What is the goal of the ReMoD therapy concept?
The ReMoD therapy concept aims at (re) learning a largely symmetrical gait pattern. This symmetrical movement forms an ideal fit with the anatomy of the human body. The human body by itself was initially not affected by hemiparesis. By (re-) learning a gait pattern that is as symmetrical as possible, long-term damage to the anatomical structures and thus severe pain and damage for the patient can be avoided.
Building blocks of the ReMoD therapy concept
The ReMoD therapy concept includes two major components in order to be able to effectively support people with hemiparesis and other vascular disorders in reaching the therapy goal at all levels. These two components are on one hand the walking aid ReMoD V5.0, and on the other hand the ReMoD Therapy concept. This way, both the sensory and motor limitations, can be treated.
Part 1 – The Sensory system
The first component presented in this text is a walking aid. The sensory system, primarily proprioceptor, vestibular visual and haptic sensory impressions provide information about the current position of the body in space the movement in space. The presence of this information / signal is a prerequisite for any walking movement. For hemiparesis patients, these signals and their transmission to the rest of the body are disturbed.
The ReMoD walking aid provides the patient with the information necessary for proprioception, that is, information on the perception of body movement and position in space and their position in relation to one another. The patient thus receives the information that is missing due to his disturbed sensory system, information which is indispensable for the basis of every walking movement.
The ReMoD walking aid can be used for specific indications of hemiparesis patients and other patients with similar walking difficulties to learn to align the body symmetrically and thus acquire a balanced starting position for symmetrical gait (see passenger / locomotor, according to Perry).
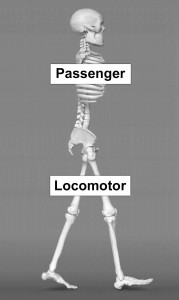
Functional division of the body
in the upper passenger and the lower locomotor
(modified from Perry 1992, p. 20)
Part 2 – The motoric system
The second component consists of a specific ReMoD training, based on the principles of biobeedback. This training is at the heart of the ReMoD rehabilitation approach. The training is individually tailored to the special needs of hemiparesis patients: impulses that are not available due to the paralysis must be replaced by alternatively available impulses or, if possible, need to be trained. In other words, our method teaches an entirely new pulse pattern, which uses those movements that the paralyzed patient can still perform.
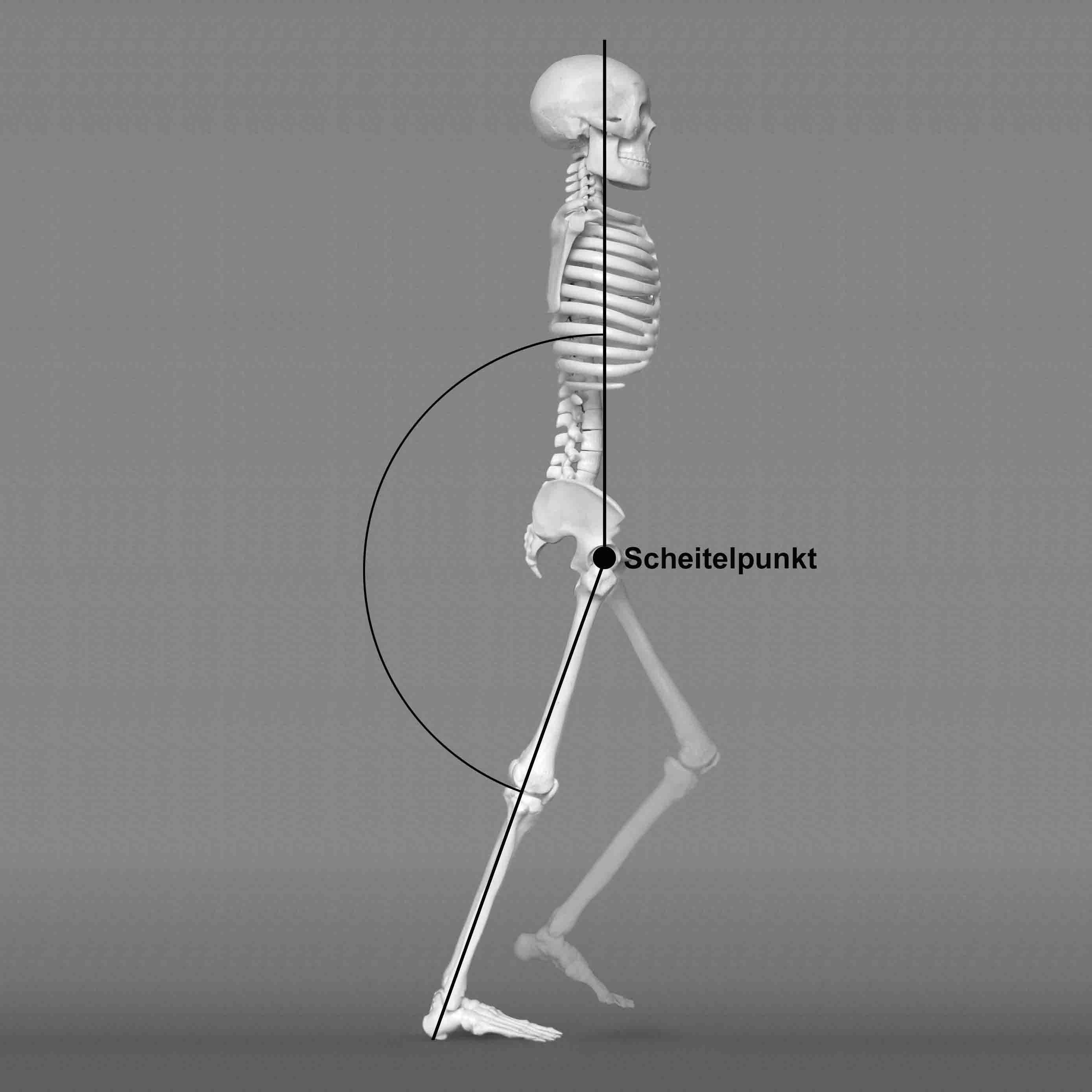
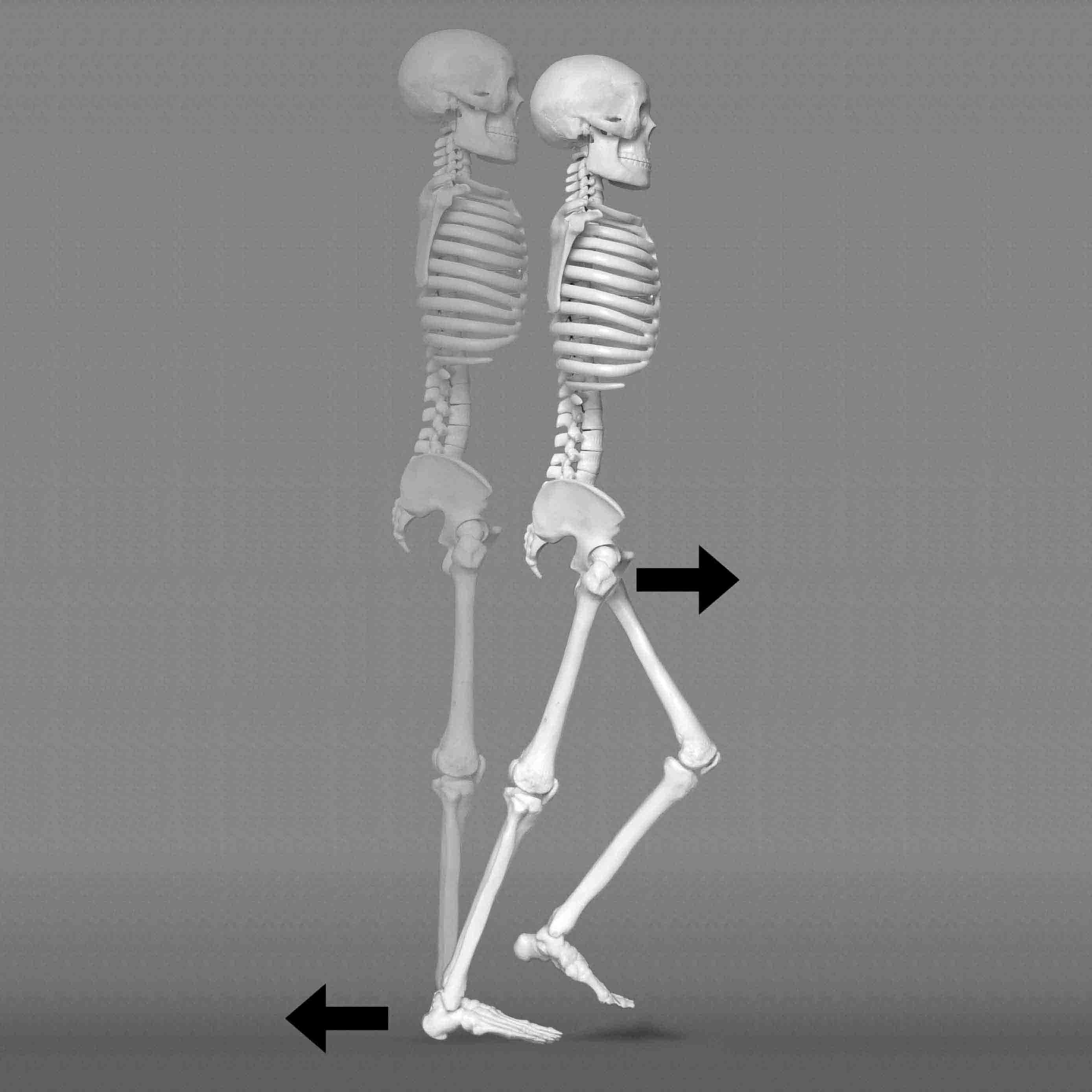
An important aspect of this training method is the diagnostic gait analysis of the hemiparetic patient, with special attention to the specific movement impulses that are required for creating or building a physiological gait.
These two building blocks were developed during the rehabilitation with Dindia Gutmann. Her almost sensational success in learning alternative movements, which has helped her to walk almost symmetrically and thus enables her to experience pain-free mobility, gives us hope that we can help other patients, too.
For a better understanding, the building blocks of the ReMoD concept are described in more detail below. Linked to this is the hope that the physiotherapeutic and movement therapy experts will take up these new kinds of building blocks and develop them further.


Our training instructions „Walking training for hemiparesis patients“ accompany the work with our biofeedback device ReMoD V5.0 Type 1
 These training instructions are at the heart of the ReMoD rehabilitation approach. The training is tailored to the special needs of hemiparesis patients: impulses that are not available due to paralysis must be replaced by alternatively available impulses or, if possible, need to be trained. Hence it’s about training an entirely new pulse pattern.
These training instructions are at the heart of the ReMoD rehabilitation approach. The training is tailored to the special needs of hemiparesis patients: impulses that are not available due to paralysis must be replaced by alternatively available impulses or, if possible, need to be trained. Hence it’s about training an entirely new pulse pattern.
You can now order our book „Angewandte Biomechanik: Gehtraining für Hemiparesepatienten” (engl: „Applied Biomechanics: Walking Training for Hemiparesis Patients“ from Vonnemann / Holodynski in bookstores. The edition is 204 pages long and is illustrated with extensive images.
Currently our book is only available in German!
Prices: Hardcover: (ISBN: 978-3746059037) € 48.99 per copy plus shipping
Paperback: (ISBN: 978-3746078700) € 24.98 per copy plus shipping

Dindia – A case study
Dindia Gutmann is paralyzed on one side as a result of a stroke at birth and suffers from spastic hemiparesis. The consequences of the paralysis meant progressive immobility. As a result, she had to be increasingly hospitalized, mostly due to inflammation in the gastrointestinal tract and severe dizziness with frequent falls. The spastic convulsions intensified over the years and occurred several times a day from age 11 on.
Dindia could only walk distances between 50 and 200 meters at the age of 11 years. She was mainly transported in a buggy. A wheelchair was inevitable due to her increasing weight. Dindia was considered beyond treatment. Doctors ruled out the possibility of an improvement in her condition.
In the hope of avoiding a life in a wheelchair, in 2002 at the age of 12 Dindia began daily movement training that closely followed the laws of biomechanics. Alongside this an electronic device for motion control was used. Both movement training and the device have been continuously optimized over the years.
The progress achieved while walking led to a significant reduction of the damage caused by paralysis. Pain decreased, her overall physical health improved as well as her mental health. The daily spastic convulsions occurred only once to twice a month.
Today Dindia enjoys hiking of up to 4 hours in a day. In training she has no problem in walking up to 14 km.
Hemiparesis
Hemiparesis is often triggered by a stroke. The effects of a stroke vary widely depending on the location and size of the effected region of the brain. The degree of impairment can range from barely noticeable disturbances to moderate disabilities to permanent bed rest. Often varying degrees of hemiparesis result affecting the arms, legs, torso and lower half of the face. Initially, the paralysis is limp while later on tension in the muscles increases more and more until it is finally convulsive (spasticity).
The basic problem of hemiparesis is the damage to the nerve pathways. The exchange of information between the brain and the limbs of the paralyzed parts of the body does not work properly or not at all. Individual body parts therefore can either no longer be activated or no longer be properly activated. They are paralyzed.
This in turn leads to an abnormal gait pattern and thus the inability to walk. This movement disorder then causes consequential damages such as spasticity, irreparable joint damage and torn vertebrae. In the worst case scenario, walking may be made impossible so that the persons concerned are confined to a wheelchair. This immobility leads to other ailments – not to mention the psychosocial problems, which affects the patient and their families.
The re-learning of a normal stride and a normal posture is extremely important for hemiparetic people and especially for children. It is important to avoid secondary damage because these are usually even more serious than the paralysis itself.

Dindia Gutmann training with an early prototype
At this point we would like to point out that not every hemiparesis patient can be helped. Prerequisites for the treatability of hemiparesis patients with ReMoD include the following indicators:
– Hemiparesis must be present
– Hemiparesis must relate to the leg
– Ability to walk a few steps and standing for one moment must be present to some extent
– The patient must be capable of rehabilitation
Alternative therapies
The therapy possibilities for hemiplegia are limited. The destruction of nerve cells is irreversible. Hemiparesis in typically addressed with physiotherapy. In this form of therapy, many tools are used to actively address partial aspects of hemiplegia. Weak dorsiflexion can be alleviated with an electronic foot lifter for example. This device is also available as an implantable version.
The problem of overextension of the knee joint and pes equinus can be alleviated by way of an orthosis.
Therapeutic devices can be used to stimulate nerves and regeneration.
Special walking frames are very helpful to help patients back on their feet after a stroke.
Hippotherapy is a special form of physiotherapy. This can be very effective and has lead to amazing results just like the Bobath or Vojta therapies. Nevertheless, the main problem never goes away: the patient cannot operate and control their own movements. In addition, the patient cannot remember the results of what they have learned. Therefore the results obtained never last.
As illustrated briefly above, the possibilities of physical therapy are limited. At best, ingrained patterns of movement can to some extent be re-activated and muscles are trained and thus protected against regression. Stiffness can be relieved through exercises and severely impaired sense of equilibrium can be trained.
However, none of these therapies can bridge the interrupted communication between the brain and motor system thus enabling the patient to control his movements independently and selectively. ReMoD can fulfil these requirements.
![]()